Heart and kidney failure often coexist, requiring complex treatment decisions. This article compares the outcomes of combined heart-kidney transplant (HKTx) with kidney transplant after heart transplant (KAH), exploring survival rates, risk factors, and procedural considerations to shed light on how these two approaches differ.
Comparing HKTx and KAH: Survival Rates and Risk Factors
A study using the United Network for Organ Sharing (UNOS) database analyzed data from 2007-2016, comparing 715 HKTx patients and 130 KAH patients. A key finding was the significantly higher mortality risk for HKTx patients.
Following a mean of 3.5 years, the multivariable-adjusted analysis revealed a 4.7-fold increased risk of death for HKTx recipients compared to KAH patients. This disparity persisted even after excluding patients on dialysis before the transplant, a known mortality risk factor.
Several factors were identified as independent predictors of mortality:
- Total artificial heart: Patients with a total artificial heart prior to transplant faced a higher risk of death.
- Intra-aortic balloon pump (IABP): IABP use before transplant was associated with increased mortality.
- Implantable cardioverter defibrillator (ICD): The presence of an ICD correlated with higher death risk.
- Pre-transplant dialysis: Patients requiring dialysis before transplant experienced elevated mortality rates.
Understanding the Trends and Patient Characteristics
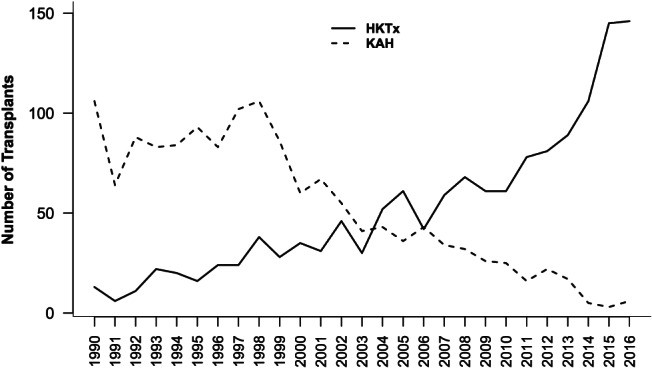
While HKTx procedures have increased in recent years, KAH procedures have declined. This could be due to evolving immunosuppression protocols, improved survival rates for dialysis patients undergoing HKTx, and the increasing use of mTOR inhibitors reducing post-transplant kidney dysfunction.
Baseline characteristics also differed between the groups. HKTx patients were generally older, more often male, and had higher serum creatinine levels, indicating poorer kidney function.
Time to Kidney Transplant in KAH Patients
In KAH patients, lower initial kidney function (estimated glomerular filtration rate – eGFR) correlated with faster listing for a kidney transplant. However, the time to needing dialysis or receiving a kidney transplant remained consistent across varying initial eGFR levels. This suggests that the cause of kidney issues after a heart transplant in KAH patients might stem from anti-rejection medications rather than pre-existing conditions.
Weighing the Pros and Cons of HKTx and KAH
HKTx Advantages:
- Potential for reduced T-cell mediated rejection, especially with organs from the same donor.
- Simultaneous correction of cardiac and renal dysfunction.
HKTx Disadvantages:
- Longer and more complex surgical procedure.
- Increased need for coordinated care between transplant teams.
- Higher mortality risk compared to KAH.
KAH Advantages:
- Option for living kidney donors, potentially improving graft survival and quality of life.
- Lower mortality risk compared to HKTx.
KAH Disadvantages:
- Requires two separate surgeries.
- Risk of developing kidney disease after the initial heart transplant due to immunosuppressants.
Conclusion: Choosing the Right Approach
While HKTx offers the advantage of addressing both heart and kidney failure simultaneously, it carries a higher mortality risk compared to KAH. KAH, though requiring two procedures, provides the possibility of a living donor and has demonstrated better survival outcomes. The decision between HKTx and KAH must be individualized, considering the patient’s specific medical condition, the availability of suitable organs, and the potential benefits and risks of each approach. Further research is crucial to refining the criteria for selecting the optimal treatment strategy.