Cardiovascular diseases (CVDs) are a leading global health concern, but how do countries with vastly different scales and healthcare systems compare in their struggle against these conditions? When we ask “How Big Is India Compared To The Usa?”, we’re not just talking about landmass, but also population size, healthcare challenges, and the sheer scale of health burdens like CVD. This article dives deep into a detailed comparison of CVD trends, risk factors, and healthcare strategies in India and the United States, revealing critical insights for global health and policy.
Understanding the Global Challenge of Cardiovascular Diseases
In 2011, the United Nations declared war on Noncommunicable Diseases (NCDs), a global effort echoed by the World Health Organization (WHO) with a target to slash premature mortality from NCDs, including CVDs, by 25% by 2025. Looking further, the UN Sustainable Development Goals push for an even more ambitious reduction of one-third by 2030. Cardiovascular health is firmly in the global spotlight, demanding effective prevention and control strategies.
Globally, the overall burden of CVD is expanding, disproportionately affecting low- and middle-income countries (LMICs) like India. This surge is primarily due to population growth and aging. Unlike high-income nations such as the United States, India has not yet seen a decline in age-adjusted CVD rates. Instead, it’s navigating an epidemiological transition, shifting from infectious diseases to NCDs. This rapid shift creates a “dual burden of disease,” presenting unique challenges across India’s diverse regions. Addressing India’s substantial CVD burden requires a deep understanding of the complex interplay of risk factors within its vast and rapidly evolving society.
This article aims to: 1) compare CVD and risk factor trends in India and the USA; 2) explore the reasons behind these differences; 3) outline current strategies in India to improve cardiovascular health; and 4) identify critical research areas for India.
CVD Trends: India and the United States Compared
Mortality and Morbidity Landscapes
CVD remains the leading cause of death in both India and the United States, mirroring global trends. In 2016, India suffered an estimated 62.5 million years of life lost prematurely to CVD, significantly higher than the 12.7 million years lost in the United States. Ischemic heart disease and stroke are major contributors, accounting for approximately 15% to 20% and 6% to 9% of all deaths in these regions, respectively.
Table 1 highlights the age-standardized CVD prevalence and estimated cases in India and the United States for 1990 and 2016. While the age-standardized prevalence of CVD was lower in India in 2016 (5,681 per 100,000) compared to the United States (7,405), India’s massive population results in a much larger absolute number of cases. In 2016, India had 54.6 million prevalent CVD cases, over 60% more than the 33.6 million in the United States.
TABLE 1. Trends in Age-Standardized Prevalence and Estimated Prevalent Cases of CVD in India and the United States
| Year | Age-Standardized Prevalence of CVD per 100,000 | Estimated No. of Prevalent Cases of CVD (Millions) |
|---|---|---|
| India | ||
| 1990 | 5,450 (95% UI: 5,256–5,657) | 25.6 (95% UI: 24.6–26.6) |
| 2016 | 5,681 (95% UI: 5,471–5,896) | 54.6 (95% UI: 52.5–56.9) |
| United States | ||
| 1990 | 8,277 (95% UI: 7,932–8,639) | 23.3 (95% UI: 22.3–24.3) |
| 2016 | 7,405 (95% UI: 7,181–7,635) | 33.6 (95% UI: 32.6–34.7) |
CVD = cardiovascular disease; UI = uncertainty interval.
CVD death rates in India are estimated to have increased from 155.7 to 209.1 per 100,000 between 1990 and 2016. However, this increase is largely attributed to population aging. Significant regional disparities exist within India, with a 9-fold difference in ischemic heart disease disability-adjusted life years (DALYs) and a 6-fold difference in stroke DALYs between states with the highest and lowest burdens. These variations likely stem from differences in risk factor prevalence, treatment access, and management of acute CVD events.
In contrast, the United States has witnessed a decline in CVD mortality, from 300 deaths per 100,000 in 1990 to 176 deaths per 100,000 in 2016 (age-standardized). However, this decline has plateaued in the last five years, a trend not fully explained by population aging.
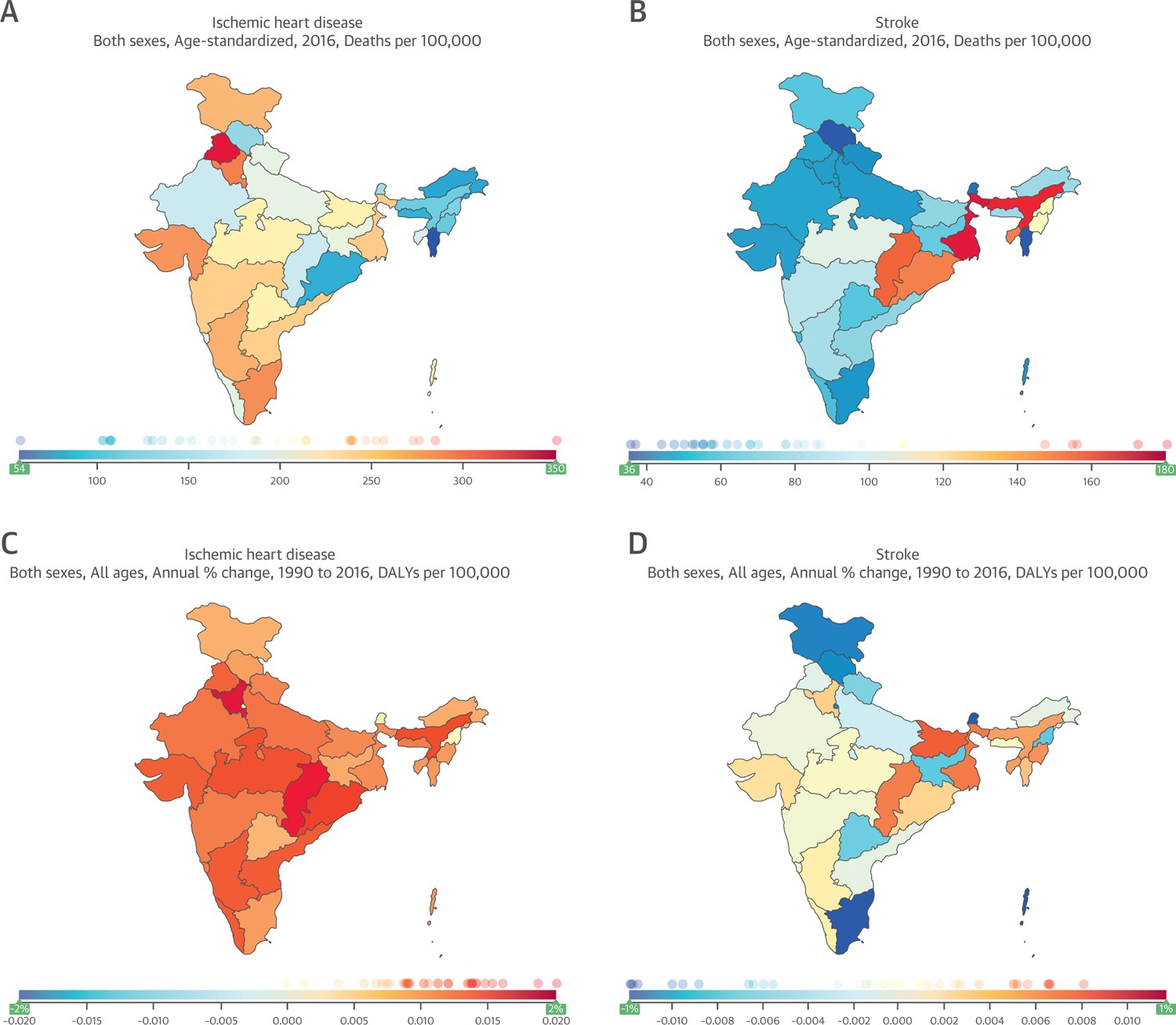
FIGURE 1.
Figure 1 illustrates the state-level variation in age-adjusted ischemic heart disease (IHD) and stroke mortality rates and DALYs per 100,000 people in India between 1990 and 2016, highlighting the diverse landscape of CVD burden across the country. Alt Text: Maps showing state-level variations in ischemic heart disease and stroke mortality rates and disability-adjusted life years (DALYs) in India from 1990 to 2016. The maps display significant differences in cardiovascular disease burden across Indian states.
CVD Surveillance Systems: A Comparative Look
Effective surveillance is crucial for managing CVD. Table 2 compares CVD surveillance methods in India and the United States. The US has comprehensive vital registration systems that accurately track deaths. India is improving its mortality data collection, but it still faces limitations. While physician-certified death records exist for urban areas, coverage remains below 30%. The India Sample Registration System, using verbal autopsy, aims to capture nationwide mortality data but is limited by potential inaccuracies and inconsistent coverage.
TABLE 2. Methods of CVD Surveillance in India and the United States
| Vital Registration | Estimated Coverage of Vital Registration | Health Examination Survey | CVD-Focused Cohort Studies | |
|---|---|---|---|---|
| India | Sample registration system, vital registration system in selected locations | 70.9% (2013)* | Yes | Yes |
| United States | Vital registration system | 99% (2015)† | Yes | Yes |
*Office of the Registrar General, India (67).
†Murphy et al. (68).
CVD = cardiovascular disease.
Both countries utilize population-based health examination surveys. India conducts several surveys like the India Annual Health Survey and the India Noncommunicable Disease Risk Factors Survey to monitor CV risk factors. However, surveillance in India is fragmented, and its national health management information system is still developing. Cohort studies, valuable for tracking risk factors and outcomes, are more prevalent in the United States. Table 3 lists major CVD studies conducted in India between 2003 and 2018.
TABLE 3. Major CVD Prevention, Treatment, and Epidemiological Studies in India Between 2003 and 2018
| Study (Ref. #) | First Author, Year | Sponsor | Design | Recruitment Location | Recruitment Period | Sample Size |
|---|---|---|---|---|---|---|
| Health promotion/primordial prevention studies | ||||||
| MYTRI (69) | Perry et al., 2009 | National Institutes of Health | Cluster RCT | Delhi and Chennai | 2004–2006 | 32 schools and 14,063 students |
| SSIP (70) | Prabhakaran et al., 2009 | World Health Organization, India, and Ministry of Health & Family Welfare, India | Pre- and postevaluation study | 10 worksites in India | 2003–2006 | 5,828 participants at baseline evaluation 6,806 participants at final evaluation |
| Primary prevention studies | ||||||
| RAPCAPS (71) | Joshi et al., 2012 | Byraju Foundation, Wellcome Trust, IC-Health | Cluster RCT | Andhra Pradesh | 2006–2008 | 1,137 high-risk individuals and 3,712 general population |
| TIPS-1 (72) | Indian Polycap Study (TIPS), 2009 | Cadila Pharmaceuticals Ltd. | Double-blind RCT | 50 centers in India | 2007–2008 | 2,053 participants |
| mPOWER Heart (73) | Ajay et al., 2016 | Medtronic Foundation | Pre- and post-intervention study | Himachal Pradesh | 2012–2014 | 6,797 participants |
| DSS-HTN, Andhra Pradesh (74) | Anchala et al., 2015 | Wellcome Trust | Cluster RCT | Andhra Pradesh | 2011–2012 | 1,638 participants |
| SMARTHealth (ongoing) (75) | Praveen et al., 2013 | National Health and Medical Research Council | Stepped-wedge cluster RCT | Andhra Pradesh | 2013–2016 | 18 primary health care clusters and 15,000 participants |
| PREPARE (ongoing) (76) | Fathima et al., 2013 | National Institutes of Health, UnitedHealth Group | Cluster RCT (household level) | Rural communities in Tamil Nadu, Karnataka, and Maharashtra | 2009–2014 | 2,438 households |
| CARRS Trial (77) | Ali et al., 2016 | National Institutes of Health | RCT | India, Pakistan | 2011–2014 | 1,146 participants |
| mWELLCARE (78) | Jha et al., 2017 | Wellcome Trust | Cluster RCT | Haryana, Karnataka | 2014–2016 | 3,600 participants |
| DISHA study (79) | Jeemon et al., 2016 | Indian Council for Medical Research | Pre- and post-intervention study | 10 sites in India | 2013–2016 | 18,000 participants (Phase1)and18,000 participants (Phase 2) |
| Secondary and tertiary prevention studies | ||||||
| ACS Kerala QI pilot program (80) | Prabhakaran et al., 2008 | World Health Organization, India, and Ministry of Health and Family Welfare, India | Pre- and post-intervention study | Kerala | 2005–2006 | Pre-intervention = 629 participants; post-intervention = 403 participants |
| UMPIRE (81) | Thom et al., 2013 | European Commission | RCT | India, Europe | 2010–2011 | 2,004 participants (1,000 in India) |
| TIPS-2 (82) | Yusuf et al., 2012 | Cadila Pharmaceuticals, Ltd. | RCT | 27 centers in India | 2010 | 518 participants |
| TIPS-3 (ongoing) (83) | NCT01646437 | Cadila Pharmaceuticals Ltd. | RCT | Karnataka | 2012–2019 | 5,713 participants (2,000 in India) |
| SIM-CARD (84) | Tian et al., 2015 | National Institutes of Health | Cluster RCT | Haryana, India; Tibet, China | 2012–2014 | 2,086 participants (1,050 in India) |
| ACS QUIK (50) | Huffman et al., 2018 | National Institutes of Health | Stepped-wedge cluster RCT | 63 hospitals in Kerala | 2014–2016 | 21,374 |
| Cardiac rehabilitation studies | ||||||
| ATTEND (85) | ATTEND Collaborative Group, 2017 | National Health and Medical Research Council | RCT | 14 hospitals in India | Jan 2014-Feb 2016 | 1,250 participants |
| Yoga-CaRe (48) | CTRI/2012/02/002408 | Medical Research Council, Indian Council for Medical Research | RCT | 25 hospitals in India | 2014–2018 | 5,000 participants |
| Eligibility Criteria | Intervention | Comparator | Follow-Up | Key Findings |
|---|---|---|---|---|
| 6th- and 8th-grade students | Multicomponent school-based intervention for tobacco cessation | No intervention | 24 months | Students in intervention group were less likely to exhibit increases in smoking |
| Adults employed at worksite and their family members | Multicomponent, multilevel intervention including posters, banners, booklets, and videos with interpersonal and environment-level foci | No intervention | NA | Significant decline in weight, waist circumference, blood pressure, plasma glucose, and total cholesterol |
| High-risk individuals and general population | Clinical algorithm-based treatment (screening of CV risk factors by trained nonphysician health workers) and health promotion | No algorithm and no health promotion | 24 months | Clinicalalgorithm-based screening ofCVriskfactors by trained nonphysician health workers identified highernumber ofindividualswithCVD risk factors and health promotion had no effect on knowledge of CVD risk factors |
| Individuals without CVD | Polycap, including aspirin, simvastatin, atenolol, ramipril, hydrochlorothiazide | 8 comparator groups of individual components of the Polycap | 12 weeks | Polycap significantly reduced multiple risk factors and CVD risk |
| Individuals with hypertension or diabetes | mHealth strategy including screening, decision support system, monitoring, and feedback tool | NA | 18 months | Nurse-facilitated, mobile phone-based clinical decision supportsystem-enabled interventionin primary care was associated with improvements in blood pressure and glucose control |
| Individuals with hypertension | Decision support system-based hypertension management | Chart-based hypertension management | 12 months | Clinical decision support is effective and cost-effective in the management of hypertension in resource-constrained primary health care settings |
| Individuals at risk of CVD | mHealth-based decision support for CVD risk factor management | No intervention | 12 months | Results pending |
| Community-dwelling participants | Household-based intervention delivered through nonphysician health workers | No intervention | 12–24 months | Results pending |
| Patients with poorly controlled type 2 diabetes | Multicomponent quality improvement strategy including nonphysician care coordinator and decision-support software | Usual care | 30 months | Intervention group had 2-fold higher likelihood of achieving risk factor goals compared with usual care |
| Patients with hypertension or diabetes | mHealth-based decision-support for hypertension and diabetes management | Usual care | 12 months | Results pending |
| Community-dwelling participants | Structured lifestyle modification delivered by frontline health workers | Usual care | 18 months | Results pending |
| Patients with ACS | Quality improvement program, service delivery package: admission orders, and discharge instructions, health education for participants | NA | 30 days | Increases in use of CVD drugs and decrease in time to thrombolysis |
| Patients with CVD | Polypill containing either aspirin, simvastatin, atenolol, lisinopril or aspirin, simvastatin, lisinopril, hydrochlorothiazide | Usual care | 18 months | 33% higher adherence to prescribed medicines in the polypill group and small but significant reductions in blood pressure and LDL cholesterol |
| Patients with CVD or at high CVD risk, including patients with diabetes | Double-dose Polycap + potassium supplementation | Single-dose Polycap | 8 weeks | Double-dose Polycap plus potassium supplementation reduced blood pressure and LDL cholesterol more than single-dose Polycap, with similar tolerability |
| Individuals at high risk of CVD but without prevalent CVD | Polycap, low-dose aspirin and vitamin D supplementation in prevention of CVD | Placebo | 5 years | Results pending |
| Individuals at high risk of CVD | Task shifting and decision support systems for lifestyle changes in high-risk patients and to improve uptake of evidence-based drugs | Usual care | 12 months | Improved quality of primary care and clinical outcomes in resource-poor settings in China and India |
| Patients with ACS | Multicomponent quality improvement toolkit | Usual care | 30 days | Improved process-of-care measures but not clinical outcomes after adjustment |
| Stroke patients with disability | Family-led rehabilitation after stroke | Usual care | 6 months | No difference in deaths or dependency found between the study groups |
| Patients with acute myocardial infarction | Yoga-based cardiac rehabilitation | Usual care | 12 months | Results pending |
| Study (Ref. #) | First Author, Year | Sponsor | Design | Recruitment Location | Recruitment Period | Sample Size |
|---|---|---|---|---|---|---|
| Registries/observational studies | ||||||
| CREATE (86) | Xavier et. al., 2008 | Sanofi-Aventis, Population Health Research Institute, St. John’s Research Institute | Registry | 50 cities in India | 2001–2005 | 20,937 participants |
| Kerala ACS registry (49) | Mohanan et al., 2013 | Cardiological Society of India, Kerala chapter | Registry | Kerala | 2007–2009 | 25,7148 participants |
| MACE registry (87) | No published reports to date | Indian Council for Medical Research | Registry | 12 hospitals in India | 2015–2018 | 3,870 participants enrolled through the end of 2017 |
| INTER-CHF registry (88) | Dokainish et al., 2016 | Novartis | Registry | Multicenter in India | 2012–2014 | 5,813 participants (2,661 in India) |
| INSPIRE (ongoing) (89) | CTRI/2013/10/004108 | National Institutes of Health | Registry | 58 hospitals in India | 2009–2012 | 10,500 participants |
| ICMR-Urban rural survey (42) | Roy et al., 2017 | Indian Council for Medical Research | Repeated cross-sectional survey | Delhi and rural Haryana | Survey 1:19911994; Survey 2: 2010 −2012 | Survey 1: 5,535 participants Survey 2: 3,969 participants |
| Jaipur Heart Watch study (90) | Gupta et al., 2003 | None reported | Cross-sectional surveys | Jaipur | First survey: 19921994; Second survey: 19992001 | 1st survey: 2,212 participants and 2nd survey: 1,123 participants |
| India Heart Watch study (91) | Gupta et al., 2015 | South Asian Society of Atherosclerosis and Thrombosis | Cross-sectional survey | 11 cities in India | 2005–2009 | 6,198 participants |
| APRHI study (92) | Joshi et al., 2006 | Byraju Foundation, George Foundation | Cause-of-death survey | Andhra Pradesh | 2003–2004 | 1,354 deaths recorded |
| PROLIFE (93) | Soman et al., 2011 | None reported | Cohort study | Kerala | 2002–2007 | 161,942 participants |
| Mumbai Cohort Study (94) | Pednekar et al., 2009 | International Agency for Research on Cancer, World Health Organization, University of Oaford | Cohort study | Mumbai | 1991–97 | 148,173 participants |
| New Delhi Birth Cohort Study (95,96) | Bhargava et al., 2004; Norris et al., 2012 | Indian Council for Medical Research, Medical Research Council, UK, and multiple sources | Cohort study | New Delhi | 1969–72 and 1998–2002 | 20,755 married women; 8,181 live births, 1,526 studied |
| Vellore Birth Cohort Study (97) | Antonisamy et al., 2009 | U.S. National Institutes of Health, Indian Council of Medical Research, and British Heart Foundation | Cohort study | Vellore, Tamil Nadu | 1969–73 and 1998–2002 | 10,670 live births |
| Pune Cohort Study (98) | Chaudhari et al., 2012 | Wellcome Trust | Cohort study | Pune | 1987–1989 | 161 |
| APCAPS (99) | Kinra et al., 2014 | Indian Council for Medical Research, Wellcome Trust, European Commission, Royal College of Physicians Eden fellowship | Cohort study | Andhra Pradesh | 2003–2005 and 2010–2012 | 6,225 participants |
| PURE (21) | Yusuf et al., 2014 | Multiple sources | Cohort study | 17 LMICs | 2003-present | 24,000 participants from India |
| CARRS Cohort study (100) | Ali et al., 2016 | National Institutes of Health | Cohort study | Delhi, Chennai, and Karachi | 2010-present | 16,288 participants |
| Eligibility Criteria | Intervention | Comparator | Follow-Up | Key Findings |
|---|---|---|---|---|
| Patients with acute myocardial infarction | NA | NA | NA | Patients with low socioeconomic position had poorer outcomes based on less favorable process-of-care measures |
| Patients with ACS | NA | NA | NA | Optimal in-hospital and discharge medical care were delivered in 40% and 46% of admissions, respectively |
| Patients with ACS | NA | NA | 6 months | Expected to provide evidence on outcomes of patients with ACS throughout India |
| Patients with acute and chronic heart failure | NA | NA | NA | Asian subjects were younger, had lower literacy levels, and were less likely to have health or medication insurance or be taking beta-blockers compared with participants from other regions, except Africa |
| Patients with acute stroke | NA | NA | NA | Results pending |
| Community-dwelling participants | NA | NA | NA | Hypertension prevalence increased from 23% to 42% and from 11% to 29% in urban and rural areas, respectively |
| Community-dwelling participants | NA | NA | NA | Diabetes prevalence = 7.8%; obesity (defined as BMI $25 kg/m2) prevalence = 33% |
| Adults 20–75 yrs of age | NA | NA | NA | Age-adjusted prevalence of diabetes = 16% |
| NA | NA | NA | NA | CVD was the leading cause of mortality (32%) |
| Community-dwelling participants | NA | NA | NA | CVD was the leading cause of mortality (40%) |
| Community-dwelling participants | NA | NA | NA | Literacy status was inversely associated with all-cause mortality |
| Infants | NA | NA | NA | An increase of 1 SD in BMI between 2 and 12 years of age was associated with an odds ratio of impaired glucose tolerance or diabetes mellitus of 1.36 |
| Infants | NA | NA | NA | Shorter maternal height was associated with IGT in young adults; IGT/diabetes and insulin resistance were associated with rapid BMI gain between childhood/adolescence and adult life |
| Infants with birth weight <2,000 g | NA | NA | Up to 18 yrs | Preterm infants had smaller head circumference, and males were short. No evidence or adiposity or hypertension was found |
| Pregnant women and children | NA | NA | NA | Socioeconomic position was directly associated with fat mass index, and inversely with central-peripheral skinfold ratio; association between socioeconomic position and other risk factors was not consistent |
| Community-dwelling participants | NA | NA | NA | CVD event rate in predominantly Indian population (low- and middle-income region) is 6.43/1,000 person-years of follow-up compared with 3.99 per 1,000 person-years of follow-up in high-income countries |
| Adults >20 yrs of age | NA | NA | NA | Behavioral risk factors, low fruit/vegetable intake, smoking, and smokeless tobacco use were more prevalent in the lowest socioeconomic status participants; weight-related risk (high BMI, high waist-to-height ratio, and prevalence of diabetes, hypertension, and dyslipidemia) was higher among high socioeconomic status participants |
Improving India’s vital registration system coverage is crucial for better surveillance. India’s National Health Policy 2017 and the National Institution for Transforming India Action Agenda 2017 to 2020 recognize the need for enhanced state-level disease surveillance, extending beyond CVD.
Cardiovascular Risk Factor Trends: A Comparison
Table 4 provides a snapshot of traditional CV risk factor trends in India and the United States. These risk factors are key drivers of CVD in both regions, as highlighted by the Global Burden of Disease (GBD) 2016 Study. Similar proportions of CVD burden are linked to high blood pressure, high cholesterol, dietary factors, tobacco use, and obesity.
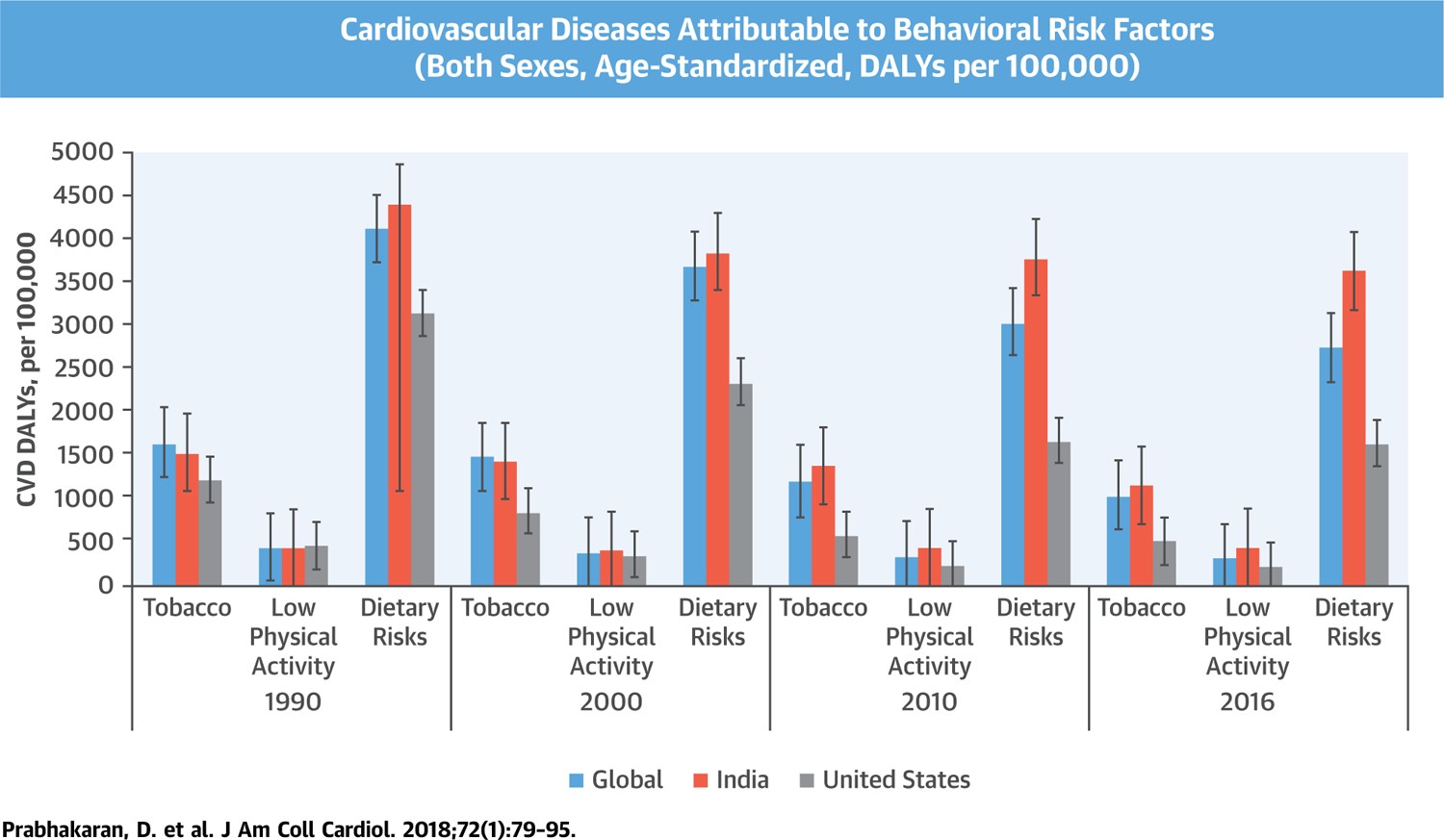
Among behavioral risk factors, dietary risks (low fruit, vegetable, grain, and nut intake; high sodium, trans-fat, and red meat consumption) are leading contributors to CVD DALYs, followed by tobacco use and physical inactivity (Central Illustration). However, among metabolic risk factors, high blood pressure and high total cholesterol are the major culprits, followed by high fasting blood glucose in India (Figure 2).
TABLE 4. Trends in Cardiovascular Risk Factors Across India and the United States
| | India | United States |
|—|—|—|—|
| | 1980 | 2015 | 1980 | 2015 |
| Tobacco use* | 17 | 10 | 30 | 13 |
| Overweight or obesity*† | 11 | 23 | 47 | 68 |
| Diabetes‡ | 3 | 9§ | 4‖ | 11 |
| Hypertension¶ | 24 | 26 | 23 | 13# |
| High total cholesterol | ** | 25††,‡‡ | 27§§,‖‖| | 12‖‖,¶¶ |
zACS = acute coronary syndrome; ACS QUIK = Acute Coronary Syndrome Quality Improvement in Kerala; APCAPS = Andhra Pradesh Children and Parents Study; APRHI = Andhra Pradesh Rural Health Initiative; ATTEND = Family-led rehabilitation after stroke in India; BMI = body mass index; BP = blood pressure; CARRS = Center for Cardio-metabolic Risk Reduction in South Asia; CREATE = Treatment and Outcomes of Acute Coronary Syndromes; CV = cardiovascular; CVD = cardiovascular disease; DISHA = Design and Rationale of a Cluster Randomised Controlled Trial; DSS-HTN = Decision Support System for Hypertension management; ICMR = Indian Council of Medical Research; IGT = impaired glucose tolerance; INTER-CHF = International Congestive Heart Failure; LDL = low-density lipoprotein; LMIC = low- and middle-income countries; MACE = major adverse cardiovascular events; mHealth = mobile (Android phone) technology–based health strategy; MYTRI = Mobilizing Youth for Tobacco-Related Initiatives in India; NA = not applicable; PREPARE = Primary pREvention strategies at the community level to Promote Adherence of treatments to pREvent cardiovascular diseases; PROLIFE = Population Registry of Lifestyle Diseases; PURE = Prospective Urban Rural Epidemiology; RAPCAPS = Rural Andhra Pradesh Cardiovascular Prevention Study; RCT = randomized controlled trial; SIM-CARD = Simplified guideline-based program for cardiovascular management by the community health workers; SSIP = Sentinel Surveillance in Indian Industrial Population; TIPS = Indian Polycap Study; UMPIRE = Use of Multidrug Pill in Reducing Cardiovascular Events; Yoga-CaRe = Yoga based Cardiac Rehabilitation Trial in India.
Values are %.
*Data from the Institute of Health Metrics and Evaluation (4).
†Defined as body mass index $25 kg/m2.
‡Data from the International Diabetes Federation (101), Global Report on Diabetes (102), NCD Risk Factor Collaboration (NCD-RisC) (103), and the CDC (104).
§These estimates are age-adjusted prevalence estimates for adults 20 to 79 years of age.
‖Aleksandrowicz et al. (7).
¶Data from the World Health Organization (105).
#These estimates are age-standardized prevalence estimates for adults ≥18 years of age, with hypertension defined as systolic blood pressure ≥140 mm Hg or diastolic blood pressure ≥90 mm Hg. For comparison, the crude 2015 hypertension estimate for U.S. adults according to the National Center for Health Statistics was 29% (Fryer et al. [106]). For this estimate, hypertension was defined as systolic blood pressure ≥140 mm Hg or diastolic blood pressure ≥90 mm Hg, or currently taking medication to lower blood pressure. Using the 2017 American College of Cardiology/American Heart Association definition of hypertension, the crude prevalence of hypertension in the United States was approximately 46% in 2011 to 2014 (Muntner P, Carey RM, Gidding S, et al. Potential U.S. population impact of the 2017 ACC/AHA high blood pressure guideline. J Am Coll Cardiol 2018;71:109–18).
**No reliable data for 1980 available. Estimate for 1993 to 1994 is 26% (106).
††Gupta et al. (107).
‡‡High cholesterol defined as total cholesterol level ≥200 mg/dl. Note: This estimate is for 2014.
§§Sempos et al. (108).
‖‖High cholesterol level defined as total cholesterol level ≥240 mg/dl.
¶¶Carroll et al. (109).
CENTRAL ILLUSTRATION.
Central Illustration: This figure visually represents the contribution of behavioral risk factors – dietary risks, tobacco use, and low physical activity – to cardiovascular disease disability-adjusted life years (DALYs) in India, the United States, and globally from 1990 to 2016. Alt Text: Bar graph comparing disability-adjusted life years (DALYs) attributable to dietary risks, tobacco use, and low physical activity for cardiovascular disease globally, in India, and the United States from 1990 to 2016. Dietary risks are shown as the largest contributor across all regions.
FIGURE 2.
Figure 2: This chart shows the CVD DALYs attributable to metabolic risk factors – high blood pressure, high cholesterol, high fasting blood glucose, and high BMI – in India, the United States, and globally from 1990 to 2016. Alt Text: Line graph illustrating disability-adjusted life years (DALYs) from cardiovascular disease attributable to metabolic risk factors (high blood pressure, high cholesterol, high fasting blood glucose, and high BMI) in India, the United States, and globally between 1990 and 2016. High blood pressure and high cholesterol are shown as the most significant metabolic risk factors.
Diabetes and chronic kidney disease contribute to atherosclerotic CVD in both India and the US. Notably, India sees a higher diabetes prevalence at a lower BMI compared to the US, resulting in comparable prevalence rates despite significant differences in average BMI. Dietary risks are similar in both countries, including low intake of fruits, vegetables, nuts, and omega-3 fatty acids, and high sodium consumption. Processed meat consumption is a greater issue in the US, while low fiber and whole grain intake is more prominent in India.
Environmental factors like ambient air pollution, persistent organic pollutants, and solid fuel exposure pose greater risks in India. Many Indian cities rank among the world’s most polluted, and despite regulations, exposure to harmful pollutants remains high. These environmental risks, linked to other NCDs, highlight the complex health challenges associated with rapid urbanization in India.
Explaining the Disparities: Why the Differences?
Upstream Social Determinants
Social determinants of health play a significant role in CVD, with extensive evidence from the US. These factors are equally relevant in India. In 1960, urban populations were 70% in the US and only 18% in India. By 2016, these figures became 82% and 33%, respectively. Rapid and uneven urbanization in India is linked to increased CVD risk factors and mortality. Lower socioeconomic status is now associated with higher CV risk factors and CVD in both regions. Socioeconomic inequalities, particularly in India, contribute to the growing CVD burden, compounded by the ongoing challenges of communicable and poverty-related diseases.
Epidemiological Transition Stages
The epidemiological transition theory explains how disease patterns change with economic development, aging, and population growth. While these factors contribute to CVD differences between India and the US, they are not universally consistent. The sociodemographic index (SDI) shows that as SDI increases, age-adjusted CVD death rates generally decline, especially between SDI 0.25 and 0.75. However, despite India’s SDI improvements, CVD mortality in men has not decreased. In the US, CVD mortality declines have plateaued recently, possibly due to obesity and diabetes, but other factors may also be at play.
Access to Quality Healthcare
While low-income countries have lower CV risk factor prevalence, they experience higher rates of major CVD events and mortality compared to high-income countries. This disparity may be due to later clinical presentation and differences in the quality of acute and chronic CVD care. For instance, in India, 80% of individuals with ischemic heart disease or stroke do not take secondary prevention medications. Even in the US, adherence to secondary prevention therapies has gaps. Regional variations in CVD within the US are partly linked to unequal access to high-quality CVD services.
Biological and Genetic Factors
Evidence suggests a higher vascular risk among native and migrant Indians compared to other ethnic groups. Factors like abdominal obesity, body fat, type 2 diabetes, and dyslipidemia may contribute to this increased CVD burden in South Asians. While the impact of CV risk factors on CVD is similar across ethnic groups, baseline CVD event rates appear higher in South Asians. Even risk thresholds, like the BMI threshold for diabetes, may be lower for South Asians. Genetic and epigenetic factors, along with early-life exposures like undernutrition, may contribute to CVD differences between India and the US. Intriguingly, studies indicate that second and third-generation South Asian immigrants in the UK have better CVD risk profiles than native white Scottish people, suggesting behavioral factors also play a role.
Infections may also be linked to CVD. For example, malaria is associated with gestational hypertension and pre-eclampsia, risk factors for low birth weight. Low birth weight is, in turn, linked to increased hypertension and ischemic heart disease risk later in life, suggesting a complex interaction between infections, birth weight, and CVD.
Strategies for a Healthier Future: Prevention and Control in India
The US has achieved significant reductions in age-adjusted CVD mortality through population-wide primary prevention and improvements in secondary and acute care. India needs to accelerate primordial, primary, secondary, and tertiary prevention efforts to reduce its CVD burden, potentially using innovative strategies to overcome resource limitations and its vast population size.
Primordial Prevention: Building a Healthy Foundation
Primordial prevention focuses on preventing risk factors from developing by promoting healthy lifestyles and behaviors. Effective and cost-effective population-wide interventions include higher tobacco taxes, advertisement bans, smoke-free policies, and reduced dietary salt intake. Banning trans fats and taxing sugary drinks are also potential policy tools. However, implementing and sustaining these policies requires strong sociopolitical will.
India ratified the WHO Framework Convention on Tobacco Control and enacted the Cigarettes and Other Tobacco Products Act, but implementation remains challenging. Pictorial warnings on cigarette packs face resistance. However, a significant excise duty increase on tobacco products in 2014 has likely contributed to declining tobacco consumption, as seen in preliminary results from the Global Adult Tobacco Survey-2 India (2016 to 2017). Access to affordable tobacco cessation drugs is limited in India, partly because they are not on the national essential medicines list.
Primary Prevention: Targeting Risk Factors
Primary prevention, focused on treating risk factors to prevent CVD, has been a major contributor to coronary heart disease mortality decline in the US. However, risk factor treatment in India is suboptimal. For example, hypertension treatment rates in India are alarmingly low compared to the US. Only 24.9% and 37.6% of diagnosed hypertensive individuals receive treatment in rural and urban India, respectively, compared to 77% in the US. Diabetes management in India is also suboptimal, with only about one-third of patients achieving adequate glycemic control, compared to 52% in the US.
To improve primary prevention in India, novel, cost-effective strategies to modify CV risk factors are essential. A 2016 analysis suggested that a benefit-based tailored treatment strategy focusing on CVD risk reduction could be more effective and cost-effective in India than current WHO-recommended strategies.
Secondary Prevention: Preventing Recurrence
Secondary prevention therapies to prevent recurrent CVD events are underutilized in India. Strategies to improve adherence in secondary prevention are similar to those in primary prevention, such as fixed-dose combination therapies, task-sharing, and integrated interventions. Table 3 lists relevant studies in India.
Cardiac rehabilitation is a crucial component of secondary prevention, reducing mortality and rehospitalization. Despite its benefits, cardiac rehabilitation is underutilized even in high-income countries and almost non-existent in India. Culturally relevant approaches like yoga-based cardiac rehabilitation may be more acceptable and effective in India. The ongoing Yoga-CaRe trial in India is evaluating the impact of yoga-based cardiac rehabilitation on clinical outcomes after acute myocardial infarction.
Tertiary Prevention: Acute Care Management
While primary and secondary prevention are key, effective management of acute CV conditions also contributes to mortality reduction. Registries in India show that acute coronary syndrome (ACS) management lags behind US standards. A 2013 registry from Kerala, a state with better health indicators, revealed areas for improvement in ACS care. The ACS QUIK trial in Kerala evaluated a quality improvement intervention to improve ACS care processes and outcomes. While the intervention improved care processes, the reduction in major adverse CV events was not statistically significant after adjusting for temporal trends. These findings provide valuable insights into acute care patterns and outcomes in Kerala, which are approaching US levels in some respects. Modeling studies suggest that expanding national insurance coverage to include CVD prevention and treatment in India would be cost-effective.
Strengthening Health Systems: The Foundation for Change
The WHO health systems framework highlights six key building blocks: service delivery, health workforce, health information systems, access to essential medicines, financing, and leadership and governance. A well-functioning health system aims for access, coverage, quality, safety, and financial risk protection.
Service Delivery: Improving Quality and Access
Health service delivery indicators include the availability and distribution of health facilities, hospital beds, and outpatient visits. These assessments are limited in India. Quality improvement initiatives for CVD care in India are still in early stages. Programs like the Tamil Nadu STEMI program, using technology to improve reperfusion therapy, show promise. Future efforts need to focus on scaling up successful initiatives, improving hospital management practices, enhancing patient-centeredness, and addressing other CV conditions like stroke and heart failure.
Health Workforce: Addressing Shortages
In 2013, there were an estimated 43 million health workers globally, but a WHO estimated shortage of 17.4 million. Distribution is uneven, both globally and within India. India has a low health worker density, with 2.1 million health workers for 1.2 billion people in 2001 (1.8 per 1,000), and a low physician-to-population ratio compared to WHO recommendations. Two-thirds of health workers are in urban areas, exacerbating shortages in rural regions where most Indians live.
Health Information Systems: Data for Action
India gathers health data through numerous agencies, but coordination and data integration are limited. Data use is also hampered by a lack of focus on outcomes and a shortage of skilled data analysts. The National Rural Health Mission’s integrated health management information system portal aims to improve data flow. India can learn from the US experience with electronic health records to create a system that truly supports patient care.
Essential Medicines: Availability and Affordability
India uses the WHO Model List of Essential Medicines as a guide. India’s generic drug industry improves the availability of essential CV drugs compared to other middle-income countries. However, affordability remains a challenge. Out-of-pocket spending on medicines is high in India, exceeding 45% of total out-of-pocket health expenses.
Financing: Investing in Health
In 2014, India’s per capita health spending was $253, 4.5% of its GDP, significantly lower than the US ($9,327, 16.6% of GDP). Government health spending in India is also proportionally lower (31.3%) compared to the US (49.8%). Out-of-pocket payments dominate health financing in India (65.6%), leading to catastrophic health spending. Increased public investment in health is crucial for India to achieve its health and economic goals.
Health Policies: Towards Universal Coverage
In the US, healthcare coverage has been mandated, although out-of-pocket costs vary. In India, healthcare is largely out-of-pocket with low insurance penetration. Lower socioeconomic groups rely on the public health system, which has limited CVD care capacity. India’s draft National Health Policy 2015 emphasizes preventive care and universal access to quality healthcare. It promotes health insurance and recommends government-funded primary care. Several health financing schemes have been launched in India, but require thorough evaluation. While private insurance can play a role, a functional public health system is essential.
Universal health coverage in India must include CVD and NCD care and provide financial protection. Cost-effectiveness analyses show that CVD care provides significant financial risk protection. Policies like tobacco taxation, salt reduction, and hypertension treatment are cost-effective and reduce both CVD and poverty in LMICs like India.
Cardiovascular Research Priorities for India
Innovation in CVD research is vital for India in five key areas:
- Robust Surveillance Systems: Establishing strong health management information systems and disease surveillance to accurately assess CVD burden and its causes.
- Policy Modeling and Evidence Synthesis: Developing health technology assessment capacity to inform evidence-based policymaking. India’s new Medical Technology Assessment Board is a step in this direction.
- Improving Access to Essential Medicines: Enhancing access to and use of essential CVD prevention drugs through task-sharing with non-physician health workers. Professional societies can play a key role in this.
- Evaluating Traditional Methods: Generating evidence on the effectiveness of traditional practices like yoga for CVD prevention and management.
- Fundamental Research: Investigating the underlying causes of high atherosclerosis rates among Asian Indians to develop targeted prevention strategies.
While the US excels in many of these areas, underserved populations and minorities also face challenges due to lack of universal healthcare and financial protection.
Conclusion: Bridging the Gap in Cardiovascular Health
The United States has significantly reduced age-adjusted CVD mortality through population-wide prevention and improvements in care. To achieve similar progress, India must implement comprehensive population-level policies while strengthening its health systems at all levels. Universal health coverage with financial risk protection is an essential goal to ensure the right to health for all Indians. Innovative research across the translational spectrum is crucial for equitable CVD prevention and control in India, with insights that can benefit global efforts.