Infants and young children are at a higher risk of respiratory complications compared to adults. This vulnerability stems from key differences in their respiratory physiology, including reflexes. This article explores these developmental differences and their implications, particularly focusing on how reflexes contribute to this increased risk.
Immature Breathing Control and Reflexes in Infants
A newborn’s breathing control system is still developing, leading to distinct breathing patterns and reflex responses compared to adults. This immaturity manifests in several ways:
- Periodic Breathing and Apneas: Infants often exhibit periodic breathing, characterized by alternating periods of rapid breathing and pauses (apneas). While generally benign, these pauses can sometimes be prolonged, leading to oxygen desaturation and bradycardia. The frequency and duration of these apneas decrease as the infant matures. Central apneas, caused by a temporary lapse in the brain’s signal to breathe, are more common in the first few weeks of life and diminish over the first year.
- Hypoxic Ventilatory Response: Unlike adults, newborns initially respond to low oxygen levels with decreased ventilation, a phenomenon known as hypoxic ventilatory depression. This counterintuitive response can worsen oxygen deprivation and highlights a crucial difference in their reflex pathways.
- Protective Reflexes: While reflexes like laryngospasm (sudden closure of the vocal cords) are present in infants, their development and sensitivity differ from adults. Research suggests a period of heightened laryngospasm risk in older infants, potentially due to ongoing neural maturation in the brainstem. The Hering-Breuer reflex, which prevents lung overinflation, is more pronounced in infants, reflecting their vulnerability to atelectasis (lung collapse).
- Trigemino-Cardiac Reflex: This reflex, triggered by stimulation of the trigeminal nerve in the face, can cause bradycardia and apnea in preterm infants, especially when a face mask is applied. This highlights the heightened sensitivity of their reflex pathways and the potential for seemingly harmless stimuli to trigger adverse events. This is related to the diving reflex, a protective mechanism that conserves oxygen during submersion in water.
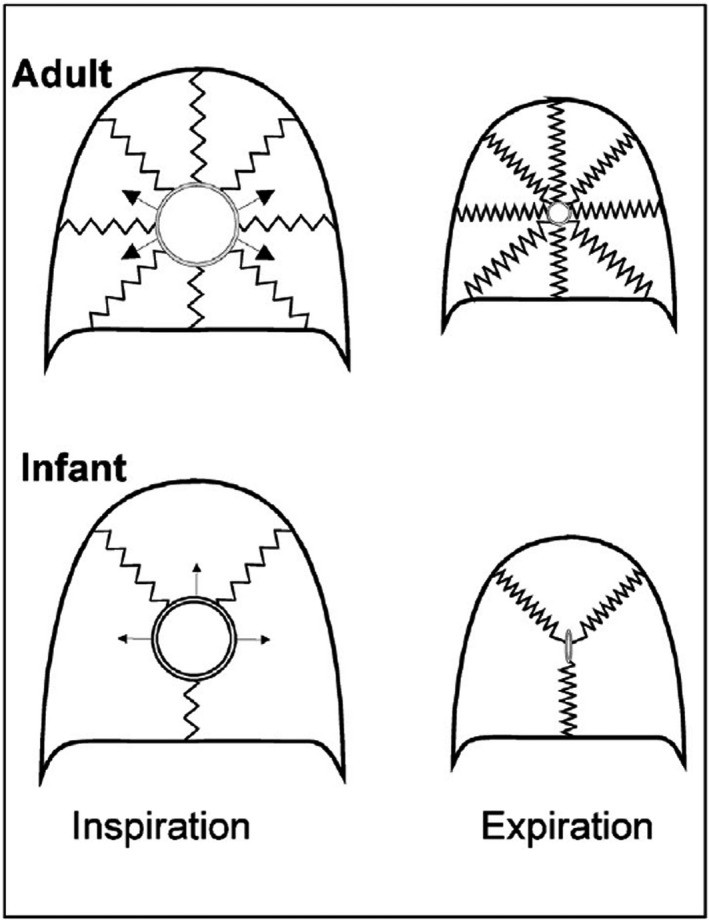 FIGURE 1
FIGURE 1
Airway Development and Reflexes
The infant airway is significantly smaller and more pliable than that of an adult, increasing susceptibility to collapse and obstruction.
- Upper Airway: The infant’s upper airway is characterized by a smaller diameter and reduced muscle tone, making it prone to collapse during inspiration. While infants possess reflexes to maintain airway patency, these mechanisms are still developing and can be easily overwhelmed. For example, simple neck flexion can induce obstructive apneas in preterm babies.
- Lower Airway: The lower airways are also smaller and less rigid, with fewer alveoli (air sacs) and less collateral ventilation (airflow between adjacent lung units). This reduced surface area for gas exchange and limited capacity to compensate for airway obstruction contribute to the infant’s respiratory vulnerability.
Anesthetic Implications of Infant Reflexes
The differences in infant reflexes have crucial implications for anesthesia administration:
- Postoperative Apnea: Infants, particularly those born prematurely, are at increased risk of postoperative apnea due to the immature control of breathing and the lingering effects of anesthetic agents.
- Airway Management: The small and collapsible airway requires careful selection of airway devices and meticulous attention to head positioning to prevent obstruction. The exaggerated trigemino-cardiac reflex necessitates gentle handling during mask ventilation.
- Respiratory Support: The propensity for atelectasis and rapid desaturation necessitates proactive respiratory support, including the use of positive end-expiratory pressure (PEEP) and careful titration of oxygen levels.
Conclusion
Infant reflexes differ significantly from those of adults, reflecting the ongoing development of their respiratory control system and airway anatomy. Understanding these differences is paramount for providing safe and effective anesthetic care to this vulnerable population. The immaturity of breathing control, heightened sensitivity to certain stimuli, and the unique characteristics of their airways contribute to the increased risk of respiratory complications in infants. Further research into the specific developmental trajectories of these reflexes will continue to improve our understanding and management of infant respiratory health.
