Height and weight comparison across different surveys provides crucial insights into population health. At COMPARE.EDU.VN, we analyze these variations to offer a comprehensive understanding. This detailed analysis helps in identifying potential biases and ensuring accurate health assessments.
Table of Contents
- What is Height Weight Compare and Why is it Important?
- How Do Different Surveys Collect Height and Weight Data?
- What Are the Key Differences in Self-Reported vs. Measured Height and Weight?
- How Does Misreporting Affect BMI and Obesity Prevalence Estimates?
- What Factors Contribute to Discrepancies in Height and Weight Data?
- Why Do NHANES, NHIS, and BRFSS Show Different Results?
- How Can Correction Methods Improve the Accuracy of Self-Reported Data?
- What are the Implications of Misreporting in Epidemiological Studies?
- How Do These Findings Inform Public Health Strategies?
- Where Can You Find Reliable Height and Weight Comparisons?
- FAQs About Height Weight Compare
1. What is Height Weight Compare and Why is it Important?
Height weight compare involves analyzing and contrasting height and weight data obtained from various sources to identify trends, discrepancies, and potential biases. This comparison is essential for accurate health assessments, epidemiological studies, and public health interventions. Understanding how height and weight measurements vary across different surveys and methodologies ensures that data-driven decisions are based on reliable information. This is especially important when tracking obesity rates and related health outcomes.
Analyzing height and weight helps in creating effective health policies and interventions. According to a study by the National Center for Health Statistics (NCHS), self-reported height and weight often differ significantly from measured values, impacting obesity prevalence estimates. By comparing data from various surveys, we can better understand these discrepancies and improve the accuracy of health statistics. This ensures that public health programs are targeted effectively and based on the most reliable data available.
2. How Do Different Surveys Collect Height and Weight Data?
Different surveys employ various methods to collect height and weight data, each with its own strengths and limitations. Understanding these methodologies is crucial for interpreting and comparing the results. Here are some common approaches:
- Measured Data (NHANES): Standardized physical examinations conducted in mobile examination centers.
- Self-Reported Data (NHANES, NHIS): In-person interviews in households.
- Telephone Interviews (BRFSS): Data collected via telephone interviews.
The National Health and Nutrition Examination Survey (NHANES) uses both measured and self-reported data, providing a benchmark for assessing the accuracy of self-reported data in other surveys. The National Health Interview Survey (NHIS) relies on in-person household interviews, while the Behavioral Risk Factor Surveillance System (BRFSS) uses telephone interviews. Each method can introduce different types of biases, such as overreporting height or underreporting weight, which need to be accounted for when comparing data.
The choice of method influences the accuracy and reliability of the data. For instance, studies have shown that participants tend to be more accurate when they know their measurements will be verified, as in NHANES. Telephone interviews, as used in BRFSS, may be subject to social desirability bias, leading to underreporting of weight and overreporting of height. Understanding these differences is crucial for interpreting and comparing data from various surveys.
3. What Are the Key Differences in Self-Reported vs. Measured Height and Weight?
Self-reported height and weight data often differ significantly from measured values, leading to potential biases in health assessments. Key differences include:
- Overreporting Height: Individuals tend to report being taller than they actually are.
- Underreporting Weight: Individuals often report weighing less than they actually do.
- BMI Discrepancies: BMI calculated from self-reported data is typically lower than BMI from measured data.
Studies consistently show that people tend to overreport their height and underreport their weight. This misreporting can lead to an underestimation of BMI and obesity prevalence. For example, research published in the American Journal of Public Health found that self-reported data underestimated obesity prevalence by as much as 20%. Understanding these discrepancies is crucial for accurate health monitoring and policy development.
The magnitude of these differences can vary by demographic factors such as age, sex, and socioeconomic status. For example, women tend to underreport their weight more than men, and older adults may have more difficulty accurately recalling their height and weight. Recognizing these patterns helps in adjusting for biases and improving the accuracy of health statistics.
4. How Does Misreporting Affect BMI and Obesity Prevalence Estimates?
Misreporting of height and weight significantly affects BMI and obesity prevalence estimates, leading to inaccurate assessments of public health. The primary impacts include:
- Underestimation of Obesity: Self-reported data often underestimates the true prevalence of obesity.
- Narrowed BMI Distribution: BMI distributions from self-reported data are narrower than those from measured data, especially at higher percentiles.
- Skewed Health Assessments: Inaccurate BMI can lead to skewed health risk assessments and inappropriate interventions.
Because individuals tend to overreport height and underreport weight, BMI calculated from self-reported data is often lower than the actual BMI. This leads to an underestimation of obesity prevalence. According to the Centers for Disease Control and Prevention (CDC), the underreporting of weight is more pronounced in women than in men, leading to greater discrepancies in obesity estimates.
The narrower BMI distribution from self-reported data also affects the accuracy of health risk assessments. Since the tails of the distribution are truncated, fewer individuals are classified as obese, which can lead to a false sense of security. This can have serious implications for public health planning and resource allocation.
5. What Factors Contribute to Discrepancies in Height and Weight Data?
Several factors contribute to discrepancies in height and weight data, including:
- Recall Bias: Difficulty accurately remembering past measurements.
- Social Desirability Bias: Reporting values that are perceived as more socially acceptable.
- Measurement Error: Inconsistencies in measurement techniques and equipment.
- Survey Methodology: Differences in data collection methods (e.g., telephone vs. in-person).
Recall bias occurs when individuals have difficulty accurately remembering their height and weight, especially over longer periods. Social desirability bias leads people to report values that align with societal norms, such as underreporting weight to avoid being seen as overweight. Measurement errors can arise from variations in measurement techniques and the use of different equipment. Additionally, the survey methodology itself can influence the accuracy of the data.
Research has shown that telephone surveys, like BRFSS, tend to yield more biased results compared to in-person surveys, like NHIS, or surveys with measured data, like NHANES. This is because telephone interviews may exacerbate social desirability bias, as respondents feel less accountable for their answers. Understanding these factors is crucial for interpreting and adjusting for biases in height and weight data.
6. Why Do NHANES, NHIS, and BRFSS Show Different Results?
NHANES, NHIS, and BRFSS often show different results due to variations in survey design, data collection methods, and target populations. Key reasons for these discrepancies include:
- Data Collection Methods: NHANES uses measured data and self-reported data, NHIS relies on in-person interviews, and BRFSS uses telephone interviews.
- Survey Design: Differences in question wording and survey administration can influence responses.
- Data Editing: Each survey employs different methods for handling extreme or missing values.
- Weighting Procedures: Variations in weighting procedures can affect the representativeness of the data.
NHANES provides a benchmark with its measured data, allowing for assessment of biases in self-reported data from NHIS and BRFSS. The use of telephone interviews in BRFSS may lead to greater social desirability bias compared to the in-person interviews used in NHIS. Additionally, differences in how extreme values are handled and how the data are weighted can contribute to variations in the results.
These differences highlight the importance of considering the methodology of each survey when comparing height and weight data. For instance, a study in the Journal of Public Health found that differences in question wording between NHIS and BRFSS led to significant variations in self-reported health status. Understanding these nuances is essential for drawing accurate conclusions and informing public health strategies.
7. How Can Correction Methods Improve the Accuracy of Self-Reported Data?
Correction methods can improve the accuracy of self-reported height and weight data by adjusting for known biases and discrepancies. Common techniques include:
- Regression Equations: Using regression equations to predict measured values based on self-reported data.
- Calibration Studies: Conducting calibration studies to quantify the differences between self-reported and measured data.
- Weighting Adjustments: Applying weighting adjustments to account for demographic and socioeconomic factors.
- Imputation Techniques: Using imputation techniques to fill in missing or unreliable data.
Regression equations are a common approach to correct for biases in self-reported data. These equations are developed using data from surveys like NHANES, which include both self-reported and measured values. By modeling the relationship between these values, researchers can predict measured values based on self-reported data.
Calibration studies involve comparing self-reported data with measured data in a subset of the population to quantify the biases. This information is then used to adjust the self-reported data in the larger survey. Weighting adjustments can account for demographic and socioeconomic factors that are associated with misreporting, such as age, sex, and education level. Imputation techniques can fill in missing or unreliable data, further improving the accuracy of the results.
8. What are the Implications of Misreporting in Epidemiological Studies?
Misreporting of height and weight in epidemiological studies can lead to biased results and inaccurate conclusions. The primary implications include:
- Biased Associations: Distorted relationships between BMI and health outcomes.
- Underpowered Studies: Reduced statistical power to detect true associations.
- Inaccurate Risk Assessments: Misleading risk assessments for obesity-related diseases.
- Ineffective Interventions: Development of interventions based on flawed data.
When BMI is calculated from self-reported data, the resulting biases can distort the relationships between BMI and health outcomes. For example, if obesity prevalence is underestimated, studies may fail to detect the true impact of obesity on diseases such as diabetes and cardiovascular disease. This can lead to inaccurate risk assessments and the development of ineffective interventions.
Additionally, misreporting can reduce the statistical power of studies, making it more difficult to detect true associations. This can result in missed opportunities to identify important risk factors and develop targeted prevention strategies. Addressing these biases is crucial for ensuring the validity and reliability of epidemiological research.
9. How Do These Findings Inform Public Health Strategies?
The findings from height weight compare studies inform public health strategies by highlighting the need for accurate data collection and analysis. Key implications include:
- Improved Data Collection: Emphasizing the use of measured data whenever possible.
- Bias Awareness: Raising awareness of the potential biases in self-reported data.
- Targeted Interventions: Developing targeted interventions based on accurate prevalence estimates.
- Enhanced Monitoring: Improving monitoring of obesity trends and related health outcomes.
Public health agencies can use the insights from these studies to improve data collection practices. For instance, prioritizing the collection of measured data, as in NHANES, can provide more accurate estimates of height, weight, and BMI. Raising awareness of the potential biases in self-reported data can help researchers and policymakers interpret the results more cautiously.
Accurate prevalence estimates are essential for developing targeted interventions. By correcting for biases in self-reported data, public health agencies can better allocate resources and design programs that effectively address the needs of the population. Enhanced monitoring of obesity trends and related health outcomes can inform timely adjustments to public health strategies, ensuring that they remain effective and responsive to changing needs.
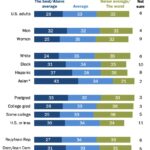
 Comparing height and weight across different demographics
Comparing height and weight across different demographics
10. Where Can You Find Reliable Height and Weight Comparisons?
Finding reliable height and weight comparisons requires accessing reputable sources of data and analysis. Here are some key resources:
- COMPARE.EDU.VN: Offers detailed comparisons and analyses of height and weight data from various surveys.
- National Center for Health Statistics (NCHS): Provides access to NHANES and NHIS data and reports.
- Centers for Disease Control and Prevention (CDC): Offers BRFSS data and related publications.
- Peer-Reviewed Journals: Publishes research articles on height weight compare and related topics.
COMPARE.EDU.VN serves as a valuable resource for accessing detailed comparisons and analyses of height and weight data. The website provides user-friendly tools and resources to help individuals and organizations make informed decisions based on reliable data.
The NCHS and CDC are primary sources for accessing raw data and reports from NHANES, NHIS, and BRFSS. These agencies also publish methodological guidelines and best practices for data collection and analysis. Peer-reviewed journals, such as the American Journal of Public Health and the Journal of Epidemiology, publish cutting-edge research on height weight compare and related topics.
11. FAQs About Height Weight Compare
Q1: Why is it important to compare height and weight data from different surveys?
Comparing height and weight data from different surveys is essential for identifying trends, discrepancies, and potential biases, ensuring accurate health assessments and effective public health interventions.
Q2: What are the main differences between self-reported and measured height and weight?
Individuals tend to overreport height and underreport weight, leading to lower BMI values calculated from self-reported data compared to measured data.
Q3: How does misreporting affect obesity prevalence estimates?
Misreporting can lead to an underestimation of obesity prevalence, affecting the accuracy of health risk assessments and the effectiveness of public health interventions.
Q4: What factors contribute to discrepancies in height and weight data?
Factors include recall bias, social desirability bias, measurement errors, and differences in survey methodology.
Q5: How can correction methods improve the accuracy of self-reported data?
Correction methods such as regression equations, calibration studies, and weighting adjustments can help adjust for known biases and discrepancies in self-reported data.
Q6: What are the implications of misreporting in epidemiological studies?
Misreporting can lead to biased associations, underpowered studies, and inaccurate risk assessments, affecting the validity of epidemiological research.
Q7: How do findings from height weight compare studies inform public health strategies?
Findings inform public health strategies by highlighting the need for accurate data collection, bias awareness, targeted interventions, and enhanced monitoring of health outcomes.
Q8: Where can I find reliable height and weight comparisons?
Reliable sources include COMPARE.EDU.VN, the National Center for Health Statistics (NCHS), the Centers for Disease Control and Prevention (CDC), and peer-reviewed journals.
Q9: What is the Behavioral Risk Factor Surveillance System (BRFSS)?
BRFSS is a state-based survey that collects data through telephone interviews regarding residents’ health-related risk behaviors, chronic health conditions, and access to health care.
Q10: How does the National Health Interview Survey (NHIS) collect height and weight data?
NHIS collects data on a broad range of health topics through in-person household interviews.
By understanding the nuances of height weight compare, you can make more informed decisions and contribute to better public health outcomes. For more detailed comparisons and analysis, visit COMPARE.EDU.VN today.
Understanding the complexities of “height weight compare” is essential for accurate health assessments and effective public health strategies. At COMPARE.EDU.VN, we provide the tools and insights you need to make informed decisions.
Ready to make informed decisions? Visit COMPARE.EDU.VN today for detailed comparisons and analyses.
For further information, please contact us at:
Address: 333 Comparison Plaza, Choice City, CA 90210, United States
WhatsApp: +1 (626) 555-9090
Website: compare.edu.vn